
Authors: Abdul Khaliq ( Department of Orthopedic and Trauma PGMI, Hayatabad Medical Complex, Peshawar. )
Imran Khan ( Department of orthopedic Gaju Khan Medical College Swabi. )
Muhammad Inam ( Department of Orthopedic and Trauma PGMI, Hayatabad Medical Complex, Peshawar. )
Mohammad Saeed ( Department of Orthopedic and Trauma PGMI, Hayatabad Medical Complex, Peshawar. )
Husnain Khan ( Department of Orthopedic and Trauma PGMI, Hayatabad Medical Complex, Peshawar. )
Malik Javed Iqbal ( Department of Orthopedic and Trauma PGMI, Hayatabad Medical Complex, Peshawar. )
November 2015, Volume 65, Issue 11
Original Article
Abstract
Objective: To compare the treatment modalities of lateral epicondylitis in terms of pain relief.
Methods: The randomised controlled study was conducted at Hayatabad Medical Complex, Peshawar, Pakistan, from April 2013 to March 2014, and comprised cases of lateral epicondylitis. The patients were selected through consecutive sampling from the outpatient department and were randomly allocated to two equal groups; group A receiving corticosteroid injections, and group B receiving injection of platelet-rich plasma. The patients were followed up for three weeks to determine the effectiveness of intervention.
Results: The 102 patients in the study were divided into two groups of 51(50%) each. The over mean age was 33.9±10.3 years. Mean age of patients in the corticosteroid group was 34.2±10.2 years and in the other group it was 33.6±10.5 years. Mean baseline visual analogue score in group A were 6.5±1.2 and in group B it was 6.7±1.4. In group A, 74.5% of patients presented in moderate pain category and 25.5% presented in severe pain category. In group B, 70.6% presented in moderate with 29.4% presented in severe pain category. On follow-up, the mean pain score in group A was 4.0±2.6 and in group B it was 3.5±2.61. Group A showed effectiveness in 52.9% patients and group B showed effectiveness in 82.3% (p=0.001).
Conclusion: PRP is an effective alternate to corticosteroid in the treatment of lateral epicondylitis (tennis elbow).
Keywords: Lateral epicondylitis, Tennis elbow, Steroid, Platelet-rich plasma, Visual analogue scale. (JPMA 65: S-100 (Suppl. 3); 2015)
Introduction
Lateral epicondylitis (LE), commonly known as tennis elbow, is a common condition that causes pain on the lateral aspect of the elbow, especially during gripping.1 Tennis elbow is commonly associated with obesity, smoking and physical loading during activity, as well as in those playing tennis.1 Epicondylitis has been associated with prolonged absence from work due to sickness in 5% of affected working-aged adults.2 LE is relatively common with an annual incidence in the general population of 1-3%.3
There are many modes of conservative treatments, including rest, alteration of tasks performed by the patient, splinting, massage, non-steroidal anti-inflammatory drugs (NSAIDs) and local steroid injection.1 Although steroid injections are widely used for treatment of chronic tennis elbow, but there are recent multiple controlled trials which support the use of platelet-rich plasma (PRP).4 After 6 months of the PRP injection, the morphology of the tendon improved when assessed using ultrasound imaging.5
PRP is prepared by centrifuging autologous, whole-blood composed of 3-8 times the concentration of platelets contained in whole blood.6 It contains autologous growth factors which help promote angiogenesis, and can promote an increased blood supply to the injured area.6 Thus, PRP injection is a relatively simple and minimally invasive method of using autologus blood-derived growth factors to promote healing.7 Treatment of LE patients with PRP reduces pain and significantly increases function, exceeding the effect of corticosteroid injection.8
Though LE is a common disease and effectiveness of PRP in its treatment is internationally proven, conflict exists between orthopaedic surgeons in Pakistan with regards to treatment for chronic LE. There is no published study to assess PRP effectiveness or to compare its results with corticosteroid injection in LE. As such, the current study was planned to compare the LE treatment modalities in terms of pain relief.
Patients and Methods
The double blind randomised controlled study was conducted at Hayatabad Medical Complex, Peshawar, Pakistan, from April 2013 to March 2014, and comprised LE patients who were selected in a consecutive manner from the outpatient department (OPD) using purposive, non-probability sampling technique. Patients having history of prior surgery of elbow, dislocation, tendon ruptures, fractures, cervical, shoulder and wrist pathology, local skin infection or osteomyelitis, rheumatoid arthritis, osteoarthritis (detected by clinical and radiological examination), metabolic diseases (diabetes, osteoporosis, osteomalacia) and neurological diseases were excluded.
After permission from the institutional ethics committee, the degree of pain in each patient at baseline was assessed using visual analogue scale (VAS) (0= no pain; 1-3 = mild pain; 4-6 = moderate pain; 7-10 = severe pain). The patients were then randomised using the toss method to two equal groups. injections. Patients in group A were injected with 2ml of methylprednisolone acetate plus 1ml of 2% xylocaine around the lateral epicondyle region. In group B, 3ml of PRP was injected in the same location. In both groups peppering technique was used to inject the autologous blood which involves inserting the needle into the tendon, injecting some of the blood, withdrawing without emerging from the skin, slightly redirecting and reinserting.
After the injection, patients in both groups were kept for 30 min under observation in the OPD for hemodynamic stability and were then discharged. All patients in both groups were re-assessed at 3 weeks to determine the effectiveness in terms of improvement in at least one grade of pain on VAS.
Data was analysed using SPSS 17. Descriptive statistics was used to calculate mean and standard deviation (SD) of age. Frequency and percentage was calculated for gender, affected side and efficacy. Efficacy in both groups was compared by using chi square test and p<0.05 was considered significant. Efficacy in both groups was stratified in terms of age, gender and baseline pain.
Results
The 102 patients in the study were divided into two groups of 51(50%) each. The overall mean age of patients in both groups was 33.9±10.3 years (range: 17.4-50.5 years). The mean age of patients in group A was 34.2±10.2 years and in group B it was 33.6±10.5 years (p=0.783).
There were 47% males and 53% females in group A and 41.2% males and 58.8% females in group B (p=0.55).
In group A, the mean baseline VAS was 6.5±1.2 and in group B it was 6.7±1.4 (p=0.519). In group A, 74.5% patients presented in moderate pain category and 25.5% in severe pain category. In group B, 70.6% presented in moderate with 29.4% presenting in severe pain category (p=1.00).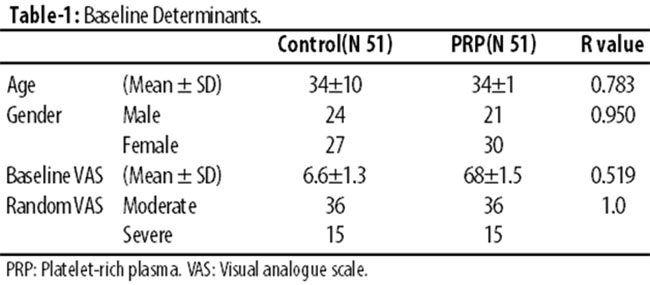
On follow up, the mean VAS score in group A was 4.0±2.6 and in group B it was 3.5±2.61 (p=0.372). On making categories with regards to pain on VAS, most of the patients were in a pain grade below severe pain on VAS (p=0.432) (Table-2).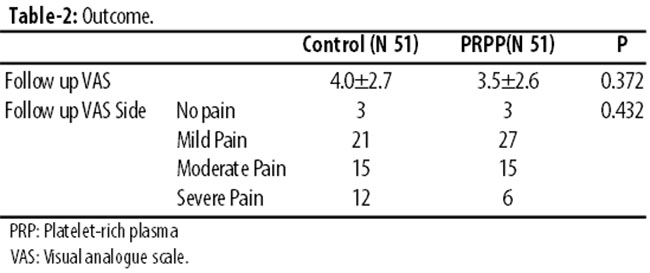
Group A showed effectiveness in 27(52.9%) patients and group B showed effectiveness in 42(82.3%) patients (Table-3).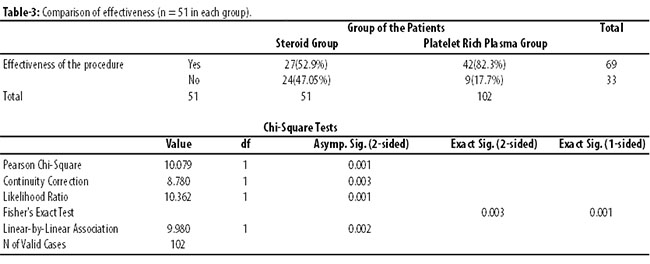
Discussion
Lateral epicondylitis (LE) or tennis elbow is an important condition of the upper extremity with an incidence of up to 4-7/1000 patients per year,9-11 having a substantial impact on athletes and workers.12 Treatment approaches for LE vary widely and lack definitive evidence.13 NSAIDs and corticosteroid injections have traditionally been used but have not been shown to be more effective than watchful waiting in the long term.14 Eccentric exercise regimens have shown some efficacy compared with age-gender-activity-matched controls, though a sub-cohort of patients remain refractory.15 Other non-surgical therapies have been evaluated for LE refractory to such conservative measures; none have been shown to be consistently effective.16 Polidocanol, prolotherapy, autologous whole blood and PRP injection therapies have reported promising outcomes for LE and other sports-related tendinopathies.17
PRP injections make use of activated platelets which discharge bioactive signalling molecules, including three adhesion molecules and seven growth factors.18 A thorough review of literature suggested that 21 of 28 clinical reports, largely from the maxillo-facial and wound-care fields, have reported positive PRP effects on bone and wound healing. However, many studies had a small sample size and used different methods for platelet processing, thereby preventing definitive conclusions.19 Most PRP-related in vitro and animal model science reports come from the orthopaedic literature on bone healing and report a variety of cellular and growth factor effects of potential importance to tendon healing.19 Studies assessing PRP effects for soft tissue healing showed increased anabolic gene expression in horse flexor tendons and proliferation of tendon cells and production of vascular endothelial growth factor (VEGF).19,21 Two large animal studies have recently reported improved healing of repaired dog and porcine cruciate ligaments following PRP therapy.19,20
The current randomised study was designed to test the use of PRP in patients with LE and proved PRP to be effective when compared with corticosteroids. There was a significant difference in decrease of pain following the platelet application after 3 weeks.
Now controversial, the corticosteroid injection was once considered the gold standard in the treatment of LE. However, studies show that it is merely the best treatment option in the short term when compared with physiotherapy and wait-and-see policy. Poor results are often seen after the 12-week follow-up.17 Treatment with corticosteroids has a high frequency of relapse and recurrence, probably because intra-tendinous injection may lead to permanent adverse changes within the structure of the tendon and because patients tend to overuse the arm after injection as a result of direct pain relief.17 In a meta-analysis, Smidt et al.21 showed that the effects of steroid injections — as compared with placebo injection, injection with local anaesthetics, injection with another steroid, or another conservative treatment — are not significantly different in the intermediate and long terms. However, the patients who were examined all had short-term LE. There are various types of surgical procedures for patients with chronic LE. Verhaar et al.22 noted an improvement in 60% to 70% of the patients after surgical treatment, although higher success rates (80% to 90%) have more recently been reported.23 Patients, however, remain interested in an alternative to surgical intervention.
In this particular study, we observed a significant difference while we compared the three-week follow-up between corticosteroids and PRP. PRP was found effective in 82.3% compared to corticosteroid injection 52.9% (p=0.001). It has been reported in literature that during the first 2 days of tendon healing, an inflammatory process is initiated by migration of neutrophils and, subsequently, macrophages to the degenerative tissue site. In turn, activated macrophages release multiple growth factors, including platelet-derived growth factor, transforming growth factors alpha and beta, interleukin-1, and fibroblast growth factor.17 Angiogenesis and fibroplasia start shortly after day 3, followed by collagen synthesis on days 3 to 5. This process leads to an early increase in tendon breaking strength, which is the most important tendon healing parameter, followed by epithelisation and, ultimately, the remodelling process.24
The results of the present study confirm the suggested positive effect in vivo as described by Mishra et al.4 They reported a significant improvement of symptoms after 8 weeks in 60% patients treated with PRP versus 16% patients treated with a local anaesthetic. After 6 months, the improvement in patients treated with PRP was 81%. They compared PRP with a local anaesthetic, which is not an accepted treatment for LE in the Netherlands. Furthermore, they injected only 15 patients with PRP and compared them with 5 patients treated with a local anaesthetic. The study was underpowered and the patients were not randomised.
Our results confirm the results of Edwards and Calandruccio.25 They injected whole blood into LE patients. Treatment success was seen in 79% patients, but multiple injections were necessary in 32%.
Three weeks were chosen as the cut-off point to consider whether the therapy was successful or not. We know that the natural history of LE predominantly results in healed patients (80%) within 1 year, but all patients in the present study had complaints for at least 6 months. In both groups, each patient had a natural history; as such and because the population was randomized, we can expect natural history to have the same influence on both groups.
The limitation of this study is that all patients had failed previous non-surgical treatments, including prior steroid injections. Furthermore, some patients had a beneficial effect after receiving more than one injection. In our study, a single percutaneous injection of PRP or corticosteroid was used. Repeated injections might be beneficial in patients who had suboptimal results after the initial injection, although no evidence for a beneficial effect of more than one injection exists.
Among other limitations, the small sample size in each arm might have affected the results. Also, the short follow-up as per our resources might also be undertaken into account in future studies as most studies reported in literature have more than a 6-month follow-up. Also, we didn\\\'t take into account new or old cases, previously treated or not, and at the same time duration of LE which should affect the results and can be studied in much larger trials in future.
The current study describes the first comparison of PRP with corticosteroid injection as a treatment for LE. It demonstrates that a single injection of PRP improves pain more so than corticosteroid injection. These improvements were sustained over time. Perhaps for athletes it is less optimal, but all depends on the demands of the patient.
Conclusion
PRP is effective in the treatment of LE. We still recommend further research that may cover complications, have a long follow-up, large sample size and use of multiple injections to generate solid evidence in favour of PRP before recommending it for routine treatment of patients with LE.
References
1. Massy-Westropp N, Simmonds S, Caragianis S, Potter A. Autologous blood injection and wrist immobilization for chronic lateral epicondylitis. Adv Orthop 2012; 2012: 387829. doi: 10.1155/2012/387829.
2. Walker-Bone K, Palmer KT, Reading I, Coggon D, Cooper C. Occupation and epicondylitis: a population-based study. Rheumatology (Oxford) 2012; 51: 305-10.
3. Raman J, MacDermid JC, Grewal R. Effectiveness of different methods of resistance exercises in lateral epicondylosis--a systematic review. J Hand Ther 2012; 25: 5-25.
4. Mishra A, Randelli P, Barr C, Talamonti T, Ragone V, Cabitza P. Platelet-rich plasma and the upper extremity. Hand Clin 2012; 28: 481-91.
5. Chaudhury S, de La Lama M, Adler RS, Gulotta LV, Skonieczki B, Chang A, et al. Platelet-rich plasma for the treatment of lateral epicondylitis: sonographic assessment of tendon morphology and vascularity (pilot study). Skeletal Radiol 2013; 42: 91-7.
6. Nguyen RT, Borg-Stein J, McInnis K. Applications of platelet-rich plasma in musculoskeletal and sports medicine: an evidence-based approach. PMR 2011; 3: 226-50.
7. Engebretsen L, Steffen K, Alsousou J, Anitua E, Bachl N, Devilee R, et al. IOC consensus paper on the use of platelet-rich plasma in sports medicine. Br J Sports Med 2010; 44: 1072-81.
8. Peerbooms JC, Sluimer J, Bruijn DJ, Gosens T. Positive effect of an autologous platelet concentrate in lateral epicondylitis in a double-blind randomized controlled trial: platelet-rich plasma versus corticosteroid injection with a 1-year follow-up. Am J Sports Med 2010; 38: 255-62.
9. Hamilton P. The prevalence of humeral epicondylitis: a survey in general practice. J R Coll Gen Pract 1986; 36: 464-5.
10. Kivi P. The etiology and conservative treatment of humeral epicondylitis. Scand J Rehabil Med 1983; 15: 37-41.
11. Ono Y, Nakamura R, Shimaoka M, Hiruta S, Hattori Y, Ichihara G, et al. Epicondylitis among cooks in nursery schools. Occup Environ Med 1998; 55: 172-9.
12. Ritz BR. Humeral epicondylitis among gas and waterworks employees. Scand J Work Environ Health 1995; 21: 478-86.
13. Bisset L, Paungmali A, Vicenzino B, Beller E. A systematic review and meta-analysis of clinical trials on physical interventions for lateral epicondylalgia. Br J Sports Med 2005; 39: 411-22.
14. Croisier JL, Foidart-Dessalle M, Tinant F, Crielaard JM, Forthomme B. An isokinetic eccentric programme for the management of chronic lateral epicondylar tendinopathy. Br J Sports Med 2007; 41: 269-75.
15. Buchbinder R, Green SE, Youd JM, Assendelft WJ, Barnsley L, Smidt N. Shock wave therapy for lateral elbow pain. Cochrane Database Syst Rev 2005; 4: CD003524.
16. Smidt N, van der Windt DA, Assendelft WJ, Devillé WL, Korthals-de Bos IB, Bouter LM. Corticosteroid injections, physiotherapy, or a wait-and-see policy for lateral epicondylitis: a randomised controlled trial. Lancet 2002; 359: 657-62.
17. Struijs PA, Smidt N, Arola H, Dijk vC, Buchbinder R, Assendelft WJ. Orthotic devices for the treatment of tennis elbow. Cochrane Database Syst Rev 2002; 1: CD00182.
18. Everts PA, Knape JT, Weibrich G, Schönberger JP, Hoffmann J, Overdevest EP, et al. Platelet-rich plasma and platelet gel: a review. J Extra Corpor Technol 2006; 38: 174-87.
19. Anitua E, Andía I, Sanchez M, Azofra J, del Mar Zalduendo M, de la Fuente M, et al. Autologous preparations rich in growth factors promote proliferation and induce VEGF and HGF production by human tendon cells in culture. J Orthop Res 2005; 23: 281-6.
20. Murray MM, Spindler KP, Abreu E, Muller JA, Nedder A, Kelly M, Collagen-platelet rich plasma hydrogel enhances primary repair of the porcine anterior cruciate ligament. J Orthop Res 2007; 25: 81-91.
21. Smidt N, Assendelft WJ, van der Windt DA, Hay EM, Buchbinder R, Bouter LM. Corticosteroid injections for lateral epicondylitis: a systematic review. Pain 2002; 96: 23-40.
22. Thomas S, Broome G. Patient satisfaction after open release of common extensor origin in treating resistant tennis elbow. Acta Orthop Belg 2007; 73: 443-5.
23. Verhaar J, Walenkamp G, Kester A, Van-Mameren H, van der Linden T. Lateral extensor release for tennis elbow: a prospective long-term follow-up study. J Bone Joint Surg Am 1993; 75: 1034-43.
24. Aspenberg P, Virchenko O. Platelet concentrate injection improves Achilles tendon repair in rats. Acta Orthop Scand 2004; 75: 93-9.
25. Edwards SG, Calandruccio JH. Autologous blood injections for refractory lateral epicondylitis. J Hand Surg Am 2003; 28: 272-8.
Journal of the Pakistan Medical Association has agreed to receive and publish manuscripts in accordance with the principles of the following committees: