
Anwarul Haque ( Aga Khan University Hospital, Karachi. )
Naveed-ur-Rehman Siddiqui ( Aga Khan University Hospital, Karachi. )
Raman Kumar ( Aga Khan University Hospital, Karachi. )
Mehar Hoda ( Aga Khan University Hospital, Karachi. )
Gulzar Lakahni ( Aga Khan University Hospital, Karachi. )
Khairunnisa Hooda ( Aga Khan University Hospital, Karachi. )
June 2015, Volume 65, Issue 6
Original Article
Abstract
Objective: To assess the cost of treatment for families of children hospitalised in paediatric intensive care unit of a tertiary care teaching hospital.
Methods: The retrospective cohort study was conducted in Aga Khan University Hospital, Karachi, and comprised record of all children admitted to the paediatric intensive care unit from January 1 to June 30, 2013. Demographic data, diagnosis at the time of admission, co-morbidity, length of stay in intensive care and outcome were recorded. The record of all hospital charges for each day the patient was cared for were also recorded. The finance department itemised the cost into major categories like pharmacy, radiology, laboratory, etc. SPSS 19 was used for statistical analysis.
Results: Record of 148 patients represented the study sample. Of them, 98(66%) were males. Overall median age was 2.7 yrs (interquartile range: 1 month to 16 years) and 93(62.8%) were below 5 years of age. Median length of stay was 3.5 days (range: 2-5 days) and total patient days in intensive care were 622. The median cost per admission was PKR 217,238 (range: (114,550-368,808) and mean cost per day was PKR 57,535 (43,911-85,527). The major cost distributions were bed charges PKR 8,092,080 (18.02%), physician charges PKR 6,398653(14.25%), medical-surgical supplies PKR 8,000772(17.8%), laboratory charges PKR 8,403,615(18.9%) and pharmacy charges PKR 5,852.226(13.03%).
Conclusion: The cost of paediatric intensive care unit was expensive. Cost distribution was almost evenly distributed. Hence, a better admission policy is needed for resource utilisation and cost-effectiveness.
Keywords: Cost, Intensive care unit, Children. (JPMA 65: 651; 2015).
Introduction
Paediatric intensive Care Units (PICUs) have contributed to health of children in developed countries.1 PICUs were recognised as a reflection of the quality of a country\'s healthcare of children.2 PICU is an essential component of children hospitals as it constitutes about 8-10% of all children hospital\'s beds.3 ICUs consume a lot of resources and are expensive. In the era of economic inflation, especially in resource-limited countries where healthcare is a self-payer, the cost evaluation is very important and vital.4,5 Numerous studies on cost of adult ICUs, both from developing and developed countries are found in literature.6-8 Multiple studies on neonatal ICUs from developing countries have been published.9 There is very little data available about cost studies in PICUs.10,11 However, there was only one publication on neonatal ICU costing from Pakistan, and none regarding the cost of PICU.12 The current study was planned to analyse the patient-related cost in PICU in terms of charges made to the family.
Patients and Methods
The retrospective cohort study was conducted after approval from the institutional review committee at Aga Khan University Hospital, Karachi, and comprised record of all children admitted to PICU for more than 24 hours from January 1 to June 30, 2013. All children admitted in PICU for more than 24 hours during the study period were included. Those re-admitted to PICU within 48 hours of PICU transfer or stay of less than 24 hours were excluded.
For the purpose of the study, PICU was defined as a separate physical facility or unit specifically designated for the treatment of paediatric patients aged from 1 month to 16-years, who, because of shock, trauma or other life-threatening conditions, require intensified, comprehensive observation and care.3 For costing , the study used a combination of "top-down" approach and "cost block method". The cost blocks include capital equipment, estates, non-clinical support services, clinical support services, consumables and staff.4-13 The first three blocks were not directly related to patients, hence they were not included. The PICU had blood gas analysis, portable radiography and ultrasound machine. The unit\'s nurse-patient ratio was 1:1 and was covered by a senior paediatric Resident round the clock under the supervision of an attending physician. Clinical data was retrospectively collected from the medical records and financial data from the hospital\'s finance department. Clinical data included basic demographic information like age and gender, primary diagnosis, co-morbidity if present, ICU therapies like use of mechanical ventilation, inotropes and renal supportive care, length of stay and outcome as \'survival\' versus \'expired\'. Data confidentiality was ensured at all stages.
There were few differences between cost and charges. We used patient\'s bill (charges) as a proxy of cost because charges bear little resemblance to economic cost.14 The hospital\'s finance department provided for each patient a record of all hospital charges for each day the patient was in PICU. The charges were also broken down into various categories like physician charges, consumable charges like medical/surgical supplies, pharmacy, radiology, laboratory and special procedure charges like surgical procedure, electrophysiological testing or plasmapharesis etc. All charges were expressed in Pakistani rupees (PKR) and converted in US dollars (USD) in accordance with the exchange rate during the study period (USD 1 = PKR 100). All charges during the stay were recorded. The cost was calculated per patient and per patient day in PICU. The data was analysed using SPSS-19. Descriptive statistics were used to describe baseline characteristics and cost data for each patient. Values were expressed as mean with standard deviation (SD) or median with interquartile range (IQR) and frequency with percentages as appropriate.
Results
Record of 148 patients represented the study sample. Of them, 98(66%) related to males. Overall median age was 2.7 years (IQR: 1 month to 16 years) and 93(62.8%) were below 5 years of age. Median length of stay was 3.5 days (IQR: 2-5 days), and total patient days in intensive care were 622. The length of stay was significantly higher in non-survivors compared to survivors (3 days vs. 5 days; p=0.04).
The case-mix consisted of 106(72.1%) medical category and 41(27.9%) surgical category. The common reasons for ICU admission were respiratory failure in 34(22.3%), trauma 21(14%), neurological illness 17(17%) and cardiac disorders 19(12.4%). Co-morbidity was found in 9(5.9%). The mortality rate was 17(11.5%) (Table-1).
The median cost per admission was PKR 217,238 (IQR: 114,550-368,808) and mean cost per day was PKR 57,535 (43,911-85,527) (Table-2).
The major cost distributions were bed charges PKR 8,092,080 (18.02%), physician charges PKR 6,398653(14.25%), medical-surgical supplies PKR 8,000772(17.8%), laboratory charges PKR 8,403,615(18.9%) and pharmacy charges PKR 5,852.226(13.03%) (Table-3, Figure).

Cost was also worked out according to the case-mix (Table-4).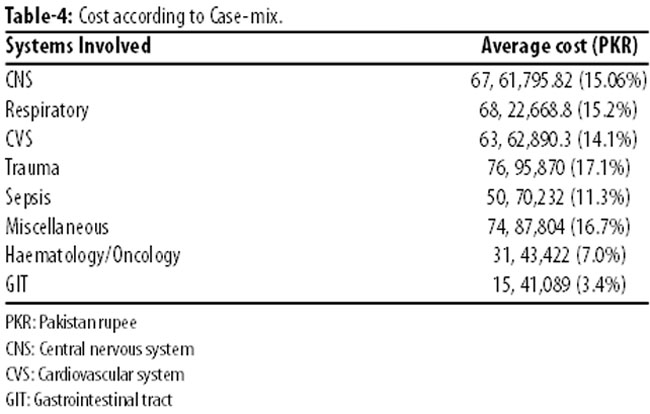
Discussions
To our knowledge, the current study is the first one to describe the cost of caring critically ill children in a PICU of a private-sector hospital of a developing country. Results suggest that the ICU care of sick child is very expensive. It was difficult to compare the data because of the limited published data on the cost of PICU. Several studies have shown that the hospitalisation of a child in PICU is a major stress for family itself. The financial stress is another major stress for parents as the costs were enormously high. There is no doubt that there is always a demand for increasing PICU beds in modern healthcare.15,16 In order to increase the size of a PICU, it is necessary to know the cost of ICU care. It is difficult to obtain the actual cost of patient care in PICU; costs were extrapolated from charges made to parents or the insurance company concerned.
Like other reports, we also found that the cost of ICU was directly related to length of stay and was higher in non-survivor\'s cases compared to those of survivors.17 Earlier studies have also shown that the cost of care is proportional to the severity of illness. One study reported that the cost of personnel was the biggest factor in intensive care.10 A significant variation in the pattern of diseases as well as distribution of cost in our cohort could not be found. However, the costs of medical-surgical supplies were higher in percentages compared to other published cost of PICU.11
There were several significant limitations to our study. This study reflects the cost of a private-sector hospital and findings cannot be generalised. A small sample size, limited period, single-centre and retrospective nature are other important weaknesses of the study. The cost blocks 1, 2 and 3 were not assessed because of difficulties. The costs were not assessed in terms of severity of illness as well as days in PICU. Most of the studies have shown that patients with high severity illness scores have longer length of stay and an increased incurred cost during these treatments.10,11 The cost on day 1 was associated with higher than cost on subsequent days.6
There are so many barriers in the care of critically ill child. However, PICUs have grown enormously in developed countries. Recent advances in medicine demand increase in the number of ICU beds. There are few solutions to this problem. First, the admission criteria for PICU should be stringent as suggested by a study in South Africa.18 Second, the public-private partnership can significantly improve the outcome. Third, there should be a structured, focused and continuous education and training on topics of critical care medicine.
Conclusion
The direct cost of critically ill or injured child in an ICU is high. There were no significant differences among the distribution of cost. The cost of ICU care of non-survivors was higher than that of the survivors. A careful selection of patients for PICU admission may lead to better utilisation of scarce resources.
References
1. Carcillo JA. What\'s new in pediatric intensive care? Crit Care Med. 2006;34:S183-90.
2. Lopez-Herce J, Sancho L, Martinon JM. Study of paediatric intensive care units in Spain. Spanish Society of Paediatric Intensive Care. Intensive Care Med. 2000;26:62-8.
3. Randolph AG, Gonzales CA, Cortellini L, Yeh TS. Growth of pediatric intensive care units in the United States from 1995 to 2001. J Pediatr. 2004;144:792-8.
4. Seidel JWP, Edbrooke DL. The Cost of intensive care. Continuing Education in Anaesthesia Crit Care Pain. 2006;6(4).
5. Jayaram R, Ramakrishnan N. Cost of intensive care in India. Indian J Crit Care Med. 2008 ;12:55-61.
6. Hariharan S, Chen D, Merritt-Charles L. Cost evaluation in the intensive care units of Trinidad applying the cost-blocks method - an international comparison. Anaesthesia. 2007;62:244-9.
7. Kulkarni AP, Divatia JV. A prospective audit of costs of intensive care in cancer patients in India. Indian J Crit Care Med. 2013;17:292-7.
8. Negrini D, Sheppard L, Mills GH, Jacobs P, Rapoport J, Bourne RS, et al. International Programme for Resource Use in Critical Care (IPOC)--a methodology and initial results of cost and provision in four European countries. Acta Anaesthesiol Scand 2006;50:72-9.
9. Prinja S, Manchanda N, Mohan P, Gupta G, Sethy G, Sen A, et al. Cost of neonatal intensive care delivered through district level public hospitals in India. Indian Pediatr;50:839-46.
10. Garcia S, Ruza F, Alvarado F, Madero R, Delgado MA, Dorao P, et al. Analysis of costs in a pediatric ICU. Intensive Care Med. 1997;23:218-25.
11. Chalom R, Raphaely RC, Costarino AT, Jr. Hospital costs of pediatric intensive care. Crit Care Med. 1999;27:2079-85.
12. Anwar Z BT. Cost of Patinet Care in Neonatal unit. J Pak Paed. 2009;33:14-8.
13. Edbrooke D, Hibbert C, Ridley S, Long T, Dickie H. The development of a method for comparative costing of individual intensive care units. The Intensive Care Working Group on Costing. Anaesthesia 1999; 54:110-20.
14. Barie PS, Ho VP. The value of critical care. Surg Clin North Am;92:1445-62.
15. Singhi S, Kissoon NN. Pediatric intensive care in India: why, how and role of global collaboration! Indian J Pediatr. 2008;75:589-90.
16. Yeolekar ME, Mehta S. ICU care in India--status and challenges. J Assoc Physicians India. 2008 ;56:221-2.
17. Shweta K, Kumar S, Gupta AK, Jindal SK, Kumar A. Economic analysis of costs associated with a Respiratory Intensive Care Unit in a tertiary care teaching hospital in Northern India. Indian J Crit Care Med 2013;17:76-81.
18. Argent AC, Ahrens J, Morrow BM, Reynolds LG, Hatherill M, Salie S, et al. Pediatric intensive care in South Africa: an account of making optimum use of limited resources at the Red Cross War Memorial Children\'s Hospital. Pediatr Crit Care Med 2014; 15:7-14.
Related Articles
Journal of the Pakistan Medical Association has agreed to receive and publish manuscripts in accordance with the principles of the following committees: