
Shumaila Arooj ( Department of Radiology, Aga Khan University Hospital, Karachi. )
Fatima Mubarak ( Department of Radiology, Aga Khan University Hospital, Karachi. )
Muhammad Azeemuddin ( Department of Radiology, Aga Khan University Hospital, Karachi. )
Zafar Sajjad ( Department of Radiology, Aga Khan University Hospital, Karachi. )
Wasey Jilani ( Department of Radiology, Aga Khan University Hospital, Karachi. )
November 2013, Volume 63, Issue 11
Case Reports
Abstract
Hirayama Disease is a disease of young adults lying in the age group between twenty to thirty years. It is an extremely uncommon disorder. Its other synonyms are juvenile muscular atrophy of the distal upper extremity(JMADUE) or monomelic amyotrophy (MMA). A previously healthy 25-year-old man presented with gradually increasing weakness in both hands for the past few years. There was neither history of trauma nor family history of neuromuscular disease. MRI was advised. Routine cervical sagittal MR images (Non-flexion or extension) revealed cord flattening and atrophy at C5 to C7 levels. There was evidence of syrinx. Flexion MRI was performed later on. Midline sagittal T1- and T2-weighted images of the cervical spine showed anterior displacement of the cervical cord with marked flattening of cord. The patient was advised to modify his posture, avoid flexion and to apply cervical collar. Physiotherapy was started to improve the tone of muscles. In case of deterioration of symptoms he was advised to consult for surgery. The purpose of this case report is to show the importance of dynamic scan in symptomatic patients especially in their second or third decade with progressive upper limb weakness. Mostly the scanning in neutral posture does not reveal any significant cord compression. Similarly a normal looking thecal sac with preserved anterior and posterior thecal sleeves without disc disease dramatically changes on change of posture. This case shows the importance of dynamic scanning in symptomatic patients with progressive upper limb weakness and with no obvious cause of the cord changes on routine MR images. Cervical collar, physiotherapy and in resistant cases surgery is recommended for management.
Keywords: Hirayama disease, Dynamic MRI, Cervical cord.
Introduction
Hirayama Disease is a disorder of young adults of the age group twenty to thirty years.1,2 It is an extremely uncommon disorder. Its other synonyms are juvenile muscular atrophy of the distal upper extremity (JMADUE)3 or monomelic amyotrophy (MMA)4 and juvenile asymmetric segmental spinal atrophy.5 Although the cause of cervical myelopathy remains unclear, neuropathologic and neuroradiologic findings suggest an abnormal compression or flattening of the anterior cord against the vertebral bodies during neck flexion, causing compression of the cervical cord, and resulting in atrophic and ischaemic changes in the anterior horn. We are reporting a case of Hirayama disease who presented in the neurology clinic with complaints of gradually increasing distal upper limb motor weakness and numbness.
Case Report
A previously healthy 25-year-old man presented with gradually increasing weakness in both hands for the past few years. He had also noticed fasiculation in his forearm and hand, along with numbness. He did not have any symptoms in lower limbs. There was neither history of trauma nor family history of neuromuscular disease. Dynamic MR examination was performed on 1.5 T Avanto 76x18 Siemens scanner in flexion and extension postures. In addition to obtaining the standard cervical spine imaging in extension, sagittal T1 and T2 weighted images in full passive flexion were also obtained. The patient while inside the scanner was instructed to gently flex his head. MR images were obtained in flexion as well as extension. Conducting the exam in multiple positions allows the spine to be assessed for mobility and angulations. Two routine (Non-flexion or extension) cervical sagittal MR images revealed cord flattening and atrophy at C5 to C7 levels. There was evidence of syrinx. Flexion MRI was performed later on. Midline sagittal T1- and T2-weighted images of the cervical spine in flexion posture showed anterior displacement of the cervical cord with marked flattening of cord. Representative MR imaging examination, with extension and flexion of the cervical spine are shown in
Figures 1a and 1b respectively. In a control patient in his second decade dynamic flexion and extension MR exam was found to be normal and there was no postural compression. Representative MR imaging examination in a control patient, with extension and flexion of the cervical spine are shown in Figures 2a and 2b,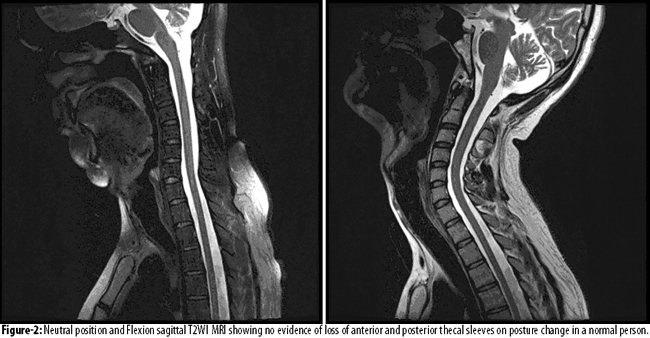
respectively.
The patient was advised to apply a cervical collar for at least 2 to 3 years since in few years there is cessation of further progression. He was also advised to modify his posture and avoid neck flexion as much as possible. Physiotherapy was started to improve muscle tone and grip. Patient and the family refused surgical intervention. They were advised to consult for surgery in case of clinical deterioration.
Discussion
The purpose of this case report is to show the importance of dynamic scanning in symptomatic patients with progressive upper limb weakness and with no obvious cause of the cord changes on routine MR images. In patients with Hirayama disease scanning in neutral posture usually does not reveal any significant cord compression. Similarly a normal looking thecal sac with preserved anterior and posterior thecal sleeves without disc disease dramatically changes on change of posture. In 1859 Hirayama Disease was reported for the first time as "juvenile muscular atrophy of distal unilateral upper extremity (JAMDUE)". From that time till now, in Asian countries including Japan as well as in European and North American countries, many young patients in the age group of twenty to thirty years presented with gradually increasing asymmetrical upper limb weakness.1 In Hirayama Disease there is predominant involvement of C7, C8 and T1 with sparing of brachioradialis which is supplied by radial nerve (C5>C6).6 This disease has a postural connection and especially related to neck flexion.7 This entity is different from disease spectrum of motor neuron diseases i-e MND in which there is involvement of both upper and lower motor neurons. The course of disease is also different and is non-progressive. The vessels of the anterior horn cells i-e the anterior spinal artery shows chronic microcirculatory changes histopathologically due to constant compression on flexion.8-10 As being described above this is due to anteriorly displaced lower cervical thecal sac in flexion resulting in atrophic asymmetric flattened cord.1,9-11 So Hirayama disease is a clearly recognized unique disease exclusively different from the typical pattern of motor neuron disease. The sooner it is detected the better is the outcome and the more effective is the treatment.1 Pardhan and Gupta from India reported the known typical MR features5 which include atrophic flattened lower cervical, asymmetrically along with abnormal cervical curvature, anterior shifting of the posterior wall of the cervical dural canal and intramedullary signal hyperintensity. Different studies also document role of applying the cervical collar for neck stabilization but is more useful in cases where the disease is detected at an earlier reversible stage.
In the early stage of Hirayama disease, the application of cervical collar is recommended.12 Cervical surgery should be carried out in some cases. It results in permanent yet long term fixation in much shorter period compared to cervical collar therapy, in which long-term application is used. This is difficult to apply long term and frequently unbearable in many patients. According to a case report, it was emphasized that operative reconstruction can be valuable, even in patients with Hirayama disease who have developed extensive intrinsic hand muscle atrophy.13
Conclusion
This case shows the importance of dynamic scanning in symptomatic patients with progressive upper limb weakness and with no obvious cause of the cord changes on routine MR images. In patients with Hirayama disease scanning in neutral posture does not reveal any significant cord compression. Similarly a normal looking thecal sac with preserved anterior and posterior thecal sleeves without disc disease dramatically changes on change of posture. Application of cervical collar stops further deterioration and flattening of cord. Avoiding flexion of neck and physiotherapy to build up tone of supporting muscles is helpful. Surgery is recommended in cases where there is deterioration in clinical condition despite supportive measures. Operative reconstruction is advantageous in cases with intrinsic hand muscle atrophy.
References
1. Hirayama K. Non-progressive juvenile spinal muscular atrophy of the distal upper limb (Hirayama\\\'s disease) In: De Jong JM, (ed.) Handbook of Clinical Neurology. Vol. 15. Amsterdam, the Netherlands: Elsevier; 1991; pp 107-20.
2. Sonwalkar HA, Shah RS, Khan FK, Gupta AK, Bodhey NK, Vottath S, et al. Imaging features in Hirayama disease. Neurol India 2008; 56: 22-6.
3. Biondi A, Dormont D, Weitzner I Jr, Bouche P, Chaine P, Bories J. MR imaging of the cervical cord in juvenile amyotrophy of distal upper extremity. AJNR Am J Neuroradiol 1989; 10: 263-8.
4. Gourie-Devi M, Suresh TG, Shankar SK. Monomelic amyotrophy. Arch Neurol 1984; 41: 388-94.
5. Pradhan S, Gupta RK. Magnetic resonance imaging in juvenile asymmetric segmental spinal muscular atrophy. J Neurol Sci 1997; 146: 133-8.
6. Tashiro K, Kikuchi S, Itoyama Y, Tokumaru Y, Sobue G, Mukai E, et al. Nationwide survey of juvenile muscular atrophy of distal upper extremity (Hirayama disease) in Japan. Amyotroph Lateral Scler 2006; 7: 38-45.
7. Hirayama K, Tokumaru Y. Cervical dural sac and spinal cord in juvenile muscular atrophy of distal upper extremity. Neurology 2000; 54: 1922-6.
8. Chen CJ, Chen CM, Wu CL, Ro LS, Chen ST, Lee TH. Hirayama disease: MR diagnosis. AJNR Am J Neuroradiol 1998; 19: 365-8.
9. Hirayama K, Tomonaga M, Kitano K, Yamada T, Kojima S, Arai K. Focal cervical poliopathy causing juvenile muscular atrophy of distal upper extremity: a pathological study. J Neurol Neurosurg Psychiatry 1987; 50: 285-90.
10. Hirayama K. Juvenile muscular atrophy of unilateral upper extremity (Hirayama disease) - half-century progress and establishment since its discovery. Brain Nerve 2008; 60: 17-29.
11. Tokumaru Y, Hirayama K. Anterior shift of posterior lower cervical dura mater in patients with juvenile muscular atrophy of unilateral upper extremity. Clin Neurol (Tokyo) 1989; 29: 1237-43.
12. Imamura H, Matsumoto S, Hayase M, Oda Y, Kikuchi H, Takano M. [A case of Hirayama\\\'s disease successfully treated by anterior cervical decompression and fusion.] No To Shinkei 2001; 53: 1033-8.
13. Chiba S, Yonekura K, Nonaka M, Imai T, Matumoto H, Wada T. Advanced Hirayama disease with successful improvement of activities of daily living by operative reconstruction. Internal Medicine 2004; 43: 79-81.
Journal of the Pakistan Medical Association has agreed to receive and publish manuscripts in accordance with the principles of the following committees: