
Nadeem Ullah Khan ( Department of Emergency Medicine, Aga Khan University Hospital, Karachi. )
Jabeen Fayyaz ( Department of Emergency Medicine, Aga Khan University Hospital, Karachi. )
Uzma Rahim Khan ( Department of Emergency Medicine, Aga Khan University Hospital, Karachi. )
Asher Feroze ( Department of Emergency Medicine, Aga Khan University Hospital, Karachi. )
November 2013, Volume 63, Issue 11
Original Article
Abstract
Objective: To assess the impact of a one-day clinical toxicology workshop in improving knowledge.
Methods: A one-day clinical toxicology workshop was conducted as a pre-conference workshop of the Annual Emergency Medicine Conference at the Aga Khan University Hospital, Karachi, in April 2012. The course was composed of poisoning-related common clinical scenarios. The pre-test and post-test understanding was used to assess the impact of the course in improving knowledge. The participants also evaluated the workshop as a whole thorough written evaluation forms. SPSS 19 was ued for statistical analysis of the data.
Result: There were 22 participants in the course. The pre-test mean score was 31.6±15.1% (95% CI; 24-40; n=19) compared to the post-test the mean score of 56.0±10.8% (95% CI; 47- 61; n=17). The positive difference was also statistically significant (p<0.001). The overall workshop was evaluated as excellent by 08 (47.46%) and very good by 10 (52.63%) participants.
Conclusion: Short training in clinical toxicology improved knowledge of the participants.
Keywords: Clinical toxicology, Emergency medicine, Teaching, Pakistan. (JPMA 63: 1379; 2013).
Introduction
Poisoning is an important cause of morbidity and mortality.1-3 It has been identified as a significant global public health problem. According to the World Health Organisation (WHO) data, an estimated 346,000 people in 2004 died worldwide from unintentional poisoning. Of these deaths, 91% occurred in low- and middle-income countries.4 Poisoning accounts for 0.86-5.9% of emergency department (ED) visits in developed countries.5 Pakistan also suffers from poisoning-related mortality and a recent study from Rawalpindi reported such deaths to be as high as 7.1%.6
Clinical toxicology focuses on the clinical presentation and management of toxic substances and associated diseases.7,8 Toxicology has now emerged as a sub-specialty of emergency medicine.9 Data has shown that toxicology-trained physicians provide a cost-effective management to patients with acute intoxication.10 In Pakistan, the initial assessment and clinical management in the ED of acutely poisoned patients are undertaken by junior physicians who do not have any formal training in clinical toxicology.11 Even patients are managed by internists with little training in toxicology. A study has shown an improvement in clinical care of acutely ill poisoned patients by targeted educational interventions.12
Formal training in toxicology like fellowship in clinical toxicology, is lacking in our undergraduate or postgraduate curricula. However, the importance of clinical toxicology has started to get recognition. The current study was aimed at assessing the impact of a short one-day course focussing on common scenarios of clinical toxicology at the ED in improving the knowledge of the participants.
Subjects and Methods
The study comprised participants of a pre-conference workshop of the Annual Emergency Medicine Conference (AEMC) 2012 held in April at the Aga Khan University Hospital. It was a one-day workshop designed to address poisoning cases and related case presenting to the ED and other important lethal poisoning of clinical significance. The course participants were Emergency physicians, General/Family Medicine practitioners and medical students.
The workshop focus was on the importance of learning clinical toxicology. General principles of poisoning management were thoroughly reviewed. Poisoning scenarios common in the region were discussed. The clinical impact of environmental and occupational hazards were also touched upon. A separate session discussed poisoning issues in children such as "One pill that can kill" and "common household poison". Most sessions were scenario-based and the mode of teaching was problem-based learning. Active participation was sought from the participants and questions and reasoning were encouraged.
Pre-test and post-test quizzes were conducted to find out the impact of the course on knowledge increase among the participants. The pre-test quiz consisted of 20 multiple choice questions (MCQs), while the post-test quiz comprised 30 MCQs. Both the quizzes comprised questions from standard text book e.g. "Tintinalli\\\'s Emergency Medicine; A Comprehensive Study Guide" and "Gold Frank\\\'s Toxicologic Emergencies".13,14 The questions were of, scenario-based "Choose the best answer", format and covered several topics (Table-1),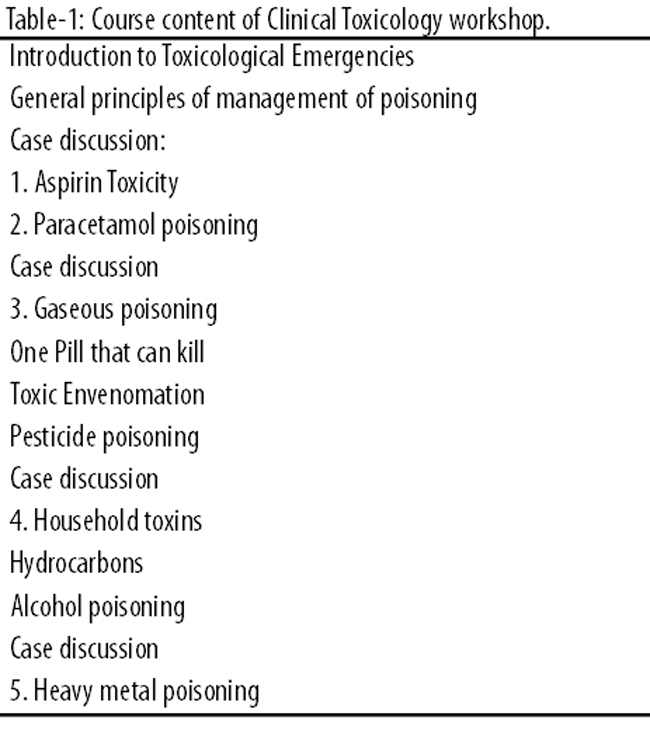
and all were MCQs (Table-2).
There was no negative marking.
At the end of the course, evaluation forms were circulated to get feedback related to the entire workshop experience. The participants were asked about objectives of the activity defined; content covered as per defined objective; overall presentation matching the participant\\\'s level of understanding; level of interaction; acquired new knowledge; time management; queries responded; organisation of the activity; quality of course material, if provided; overall assessment of the activity.
The rating of the activity was assessed on a five-point scale; excellent scored as 5, very good as 4, good as 3, average as 2; and poor as 1.
To calculate mean differences for paired observations in pre- and post-assessment scores, paired t-test was used. Confidence interval for mean scores was also calculated using t-statistics. SPSS version 19 was used to analyse the data.
Results
Of the total 22 participants pre-test and post-test quizzes were undertaken by 16 (73%), while the overall evaluation form was filled by 19 (86%). The mean score in the pre-test quiz was 31.6±15.1% (95% CI; 24-40; n=19), while in the post-test quiz the mean score was 56.0±10.8% (95% CI; 47- 61; n=17) (Table-3).
The difference was positive and statistically significant (p<0.001) (Figure).
The evaluation of the overall course was rated as \\\'excellent\\\' by 8(47.46%), \\\'very good\\\' by 10 (52.63%) and \\\'good\\\' by 1(5.26%) of the participants. No one rated the course as \\\'average\\\' or \\\'bad\\\' (Table-4).
Discussion
To the best of our knowledge, it is the first study of its kind from the country. It highlights two important facts; first, a lack of knowledge among healthcare providers with regards to clinical toxicology evident from suboptimal scores in the pre-test quiz and second, that training in clinical toxicology helps in acquiring knowledge.
Participants of the workshop included Family and Emergency physicians, who are likely to encounter cases of clinical toxicology, and the medical students, who were undergoing clinical training and should have general knowledge of the management of such cases. Poisoning kills people in the younger age group and the poisoning mortality is high in developing countries overall, including Pakistan.1,15-20 While there are various factors for this high mortality, but we assume that lack of knowledge of poisoning management could also potentially contribute.21 The reason for this lack of knowledge is limited exposure as well as opportunity during undergraduate and postgraduate training in Pakistan. A survey of academic leaders in medical college identified a perceived need of training in Emergency Medicine which will help develop the area of clinical toxicology.11
In the US, toxicology training is included in the curriculum of Emergency Medicine residency programme.22,23 They also have well-established poison control centres which offer training to both undergraduates and postgraduates, in addition to providing awareness and education to community.22,24 Some centres offer hazardous material (HazMat) life support course that are generally 2-3 days in duration and over toxicological emergencies, including chemical disaster.25 Toxicology training is also offered as a fellowship programme in the US and Master\\\'s programme in the UK.26,27 In Pakistan, there are no programmes especially designed for clinical toxicology training. Forensic Medicine as a curriculum in medical college does cover the medico-legal aspect of toxicology during undergraduate training, but clinical exposure is limited. In Pakistan there are two poison control centres, but educational opportunities available at these centres are limited.28
The results highlight that even a short training course improves knowledge significantly in this subject.29 This will potentially help in improving patient care. The course was rated highly and was appreciated by the participants. Some participants commented that this should be offered over a longer period of time.
Including clinical toxicology in the undergraduate curriculum as well as fellowship in clinical toxicology are needed and a pre-requisite for reducing the injury burden related to this preventable cause.
Conclusion
Clinical toxicology knowledge is lacking among healthcare providers. Short training course helps in improving the knowledge significantly.
Acknowledgement
We are grateful to Asher Bin Feroze for statistical assistance.
References
1. Juntti-Patinen L, Kuitunen T, Pere P, Neuvonen PJ. Drug-related visits to a district hospital emergency room. Basic Clin Pharmacol Toxicol 2006; 98: 212-7.
2. Raschetti R, Morgutti M, Menniti-Ippolito F, Belisari A, Rossignoli A, Longhini P, et al. Suspected adverse drug events requiring emergency department visits or hospital admissions. Eur J Clin Pharmacol 1999; 54: 959-63.
3. Budnitz DS, Pollock DA, Weidenbach KN, Mendelsohn AB, Schroeder TJ, Annest JL. National surveillance of emergency department visits for outpatient adverse drug events. JAMA 2006; 296: 1858-66.
4. World Health Organization. Poisoning Prevention and Management, 2004.
5. Stoukides CA, D\\\'Agostino PR, Kaufman MB. Adverse drug reaction surveillance in an emergency room. Am J Hosp Pharm 1993; 50: 712-4.
6. Khurram M, Mahmood N, Ikram N. Unintentional poisoning: experience at a medical unit. J Rawal Med Coll 2010; 14: 46-8.
7. Gossel TA, Bricker DJ. Basic principles of toxicology. In: Gossel TA, Bricker DJ (eds.). Principles of Clinical Toxicology. New York, NY: Raven Press; 2002.
8. Katzung BG, Masters SB, Trevor AJ (eds.). Basic and Clinical Pharmacology. 11th ed. New York, NY: McGraw-Hill; 2009.
9. Munger BS, Whelan GP. Role of the American Board of Emergency Medicine in the specialty of emergency medicine. Ann Emerg Med 1997; 30: 219-23.
10. Chung AHY, Tsui SH, Tong HK. The impact of an emergency department toxicology team in the management of acute intoxication. Hong Kong J Emerg Med 2007; 14: 134-43.
11. Razzak JA, Ahmed A, Saleem AF, Nasrullah M. Perceived need for emergency medicine training in Pakistan: a survey of medical education leadership. Emerg Med Australas 2009; 21: 143-6.
12. Greene SL, Wood DM, Gawarammana IB, Warren-Gash C, Drake N, Jones AL, et al. Improvement in the management of acutely poisoned patients using an electronic database, prospective audit and targeted educational intervention. Postgrad Med J 2008; 84: 603-8.
13. Tintinalli JE, Stapczynski JS, Ma OJ, Cline DM, Cydulka Rk, Meckler GD (eds.). Tintinalli\\\'s Emergency Medicine: A Comprehensive Study Guide. 7th ed. New York, NY: McGraw-Hill Medical; 2010.
14. Flomenbaum N, Goldfrank LR, Hoffman RS, Howland MA, Lewin NA, Nelson LS (eds.). Goldfrank\\\'s Toxicologic Emergencies. 8th ed. New York: McGraw-Hill Professional; 2006.
15. Tufekci IB, Curgunlu A, Sirin F. Characteristics of acute adult poisoning cases admitted to a university hospital in Istanbul. Hum Exp Toxicol 2004; 23: 347-51.
16. Murali R, Bhalla A, Singh D, Singh S. Acute pesticide poisoning: 15 years experience of a large North-West Indian hospital. Clin Toxicol 2009; 47: 35-8.
17. Shahid M, Hyder AA. Deliberate self-harm and suicide: a review from Pakistan. Int J Inj Contr Saf Promot 2008; 15: 233-41.
18. Iff, II. HEALTH HAZARDS OF PESTICIDES IN PAKISTAN. 2000.
19. Memon Y, Majeed R, Kolachi HBUX, Querashi K, Sheikh S. Clinical spectrum and outcome of accidental poisoning in children. Biomedica 2010; 26: 92-5.
20. Manzar N, Saad SM, Manzar B, Fatima SS. The study of etiological and demographic characteristics of acute household accidental poisoning in children-a consecutive case series study from Pakistan. BMC Pediatr 2010; 10:28. doi: 10.1186/1471-2431-10-28.
21. Siddiqui EU, Razzak JA, Naz F, Khan SJ. Factors associated with hydrocarbon ingestion in children. J Pak Med Assoc 2008; 58: 608-12.
22. Dart RC (ed). Medical Toxicology. Philadelphia, PA: Lippincott Williams & Wilkins; 2004.
23. Arnold JL. International emergency medicine and the recent development of emergency medicine worldwide. Ann Emerg Med 1999; 33: 97-103.
24. Burdick WP, Jouriles NJ, D\\\'Onofrio G, Kass LE, Mahoney JF, Restifo KM. Emergency medicine in undergraduate education.Acad Emerg Med 1998; 5: 1105-10.
25. Moye PK, Pesik N, Terndrup T, Roe J, Weissman N, Houston TK, et al. Bioterrorism training in US emergency medicine residencies: has it changed since 9/11? Acad Emerg Med 2007; 14: 221-7.
26. Thomas SHL. An agenda for UK clinical pharmacology: developing and delivering clinical toxicology in the UK National Health Service. Br J Clin Pharmacol 2012; 73: 878-83.
27. Tormey WP, Moore T. Poisonings and clinical toxicology: a template for Ireland. Ir J Med Sci 2013; 182: 17-23. doi:10.1007/s11845-012-0828-3.
28. Turabi A, Hasan S, Ara J, Ahmed M. Drug overdose; study conducted at National Poison Control Center. Pak J Pharmacol 2006; 23: 31-7.
29. Alsharif NZ. A standardized patient-oriented approach to teaching clinical toxicology. Am J Pharm Educ 2008; 72: 120.
Related Articles
Journal of the Pakistan Medical Association has agreed to receive and publish manuscripts in accordance with the principles of the following committees: